Prior to the prorogation of parliament, Bill S-253, which aims to establish a national framework for addressing Fetal Alcohol Spectrum Disorder (FASD) in Canada, was under review in the Senate of Canada. Key changemakers submitted briefs to the committee as part of this legislative process, outlining their support for the bill and offering valuable perspectives on improving outcomes for those with FASD. In this blog series, we will share some of these briefs to highlight the compelling reasons why Canada needs a National FASD Framework.
FASD from a Prevention Lens
This brief comes from Nancy Poole, PhD, LLD (Hon) who is the Director of the Centre of Excellence for Women and Prevention Lead at CanFASD. This brief addresses how a National FASD Framework could advance FASD prevention in Canada and highlights how important it is to see FASD prevention as a women’s health and social justice issue.
You can read the brief on the Senate of Canada’s website or read on to see the full text adapted for our blog. A French version of the document is also available on the Senate of Canada website.
Support a National FASD Framework
How can you help? Never underestimate the power of your voice! Talk to your Member of Parliament about a National FASD Framework and keep the conversation moving forward. With an election on the horizon, candidates are eager to earn your vote – seize this opportunity to make FASD a priority. Speak to them, demand action, and let them know that a National FASD Framework matters to you and your community!
Women’s Health and FASD Prevention in Canada
I am a Tahltan/Tlingit mother who looked for services and assessments when coming to terms with my alcohol consumption during my pregnancies. When I came forth to access services, I experienced judgement and stigma which made me feel unsafe. Without the guidance of FASD Advocates who supported and encouraged me to keep speaking out as a mother, I would not have followed through in getting my children diagnosed. I believe it is important that pregnant people and mothers know that there are safe, available supports that they can access. Accessibility to these supports need to come from a trauma informed lens, with a harm reduction focus, to create a culturally, emotionally, and mentally safe space. Coming forth to admit you drank in your pregnancy does not feel safe to pregnant people. As a mother and a support worker/coordinator who advocates and shares her experience and knowledge, my hope is that me sharing my story will help other pregnant parents feel safe and get the supports they need.
Based on my experience as a mother and a support worker for the past 20 years I strongly support the initiative enact a National FASD Framework.
Lisa Lawley, Shaw What Gah (Mother Wolf’s Cry)
Biological mother/Circle of Life/Perinatal Substance Use Coordinator
Canada’s Multilevel Prevention Model
In Canada we have defined and promoted a 4-level model of FASD prevention that has received global attention. Foundational to the model are structural policies related to alcohol and to maternal/child health and welfare. The four informational and care levels of this model span general and specific practices that assist women to improve their health and the health of their children, with support from family, support networks, health and social services, and community.
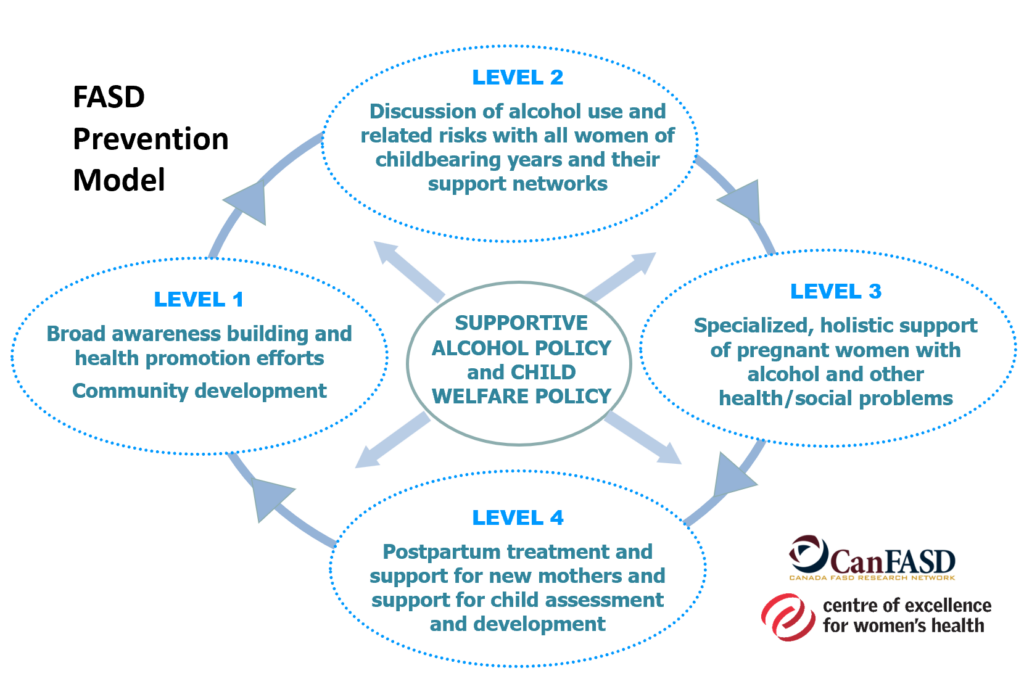
- The first level of prevention is about raising public awareness through campaigns and health promotion strategies. The inclusion of a broad range of people in community level health promotion is important to advancing social support and change. Public policy initiatives supportive of girls’ and women’s health are also key to this level of prevention. In this way, awareness of the disability, the risks of alcohol use and the evidence for compassionate support is a necessary foundation for all other levels.
- The second level is about girls, women and gender diverse individuals of childbearing years having the opportunity for safe discussions about reproductive health, contraception, pregnancy, alcohol use, and related issues, with their support networks and trusted health and social care providers.
- The third level concerns the provision of supportive services that are specialized, culturally safe and accessible for women with alcohol problems, histories of violence and trauma, and related health concerns. These trauma-informed, harm-reduction-oriented recovery services are needed not only for pregnant women, but also before pregnancy and throughout the childbearing years.
- The fourth level of prevention is about supporting new mothers to maintain healthy changes they have been able to make during pregnancy or to continue their efforts to make needed change. Postpartum support for mothers who were not able to make significant changes in their substance use during pregnancy is also vital, to assist them to continue to improve their health, social support, and where necessary, to access substance use treatment. At this level of prevention, attachment between mothers and children is promoted, child health services offered, and where necessaryF, ASD diagnostic services offered.
A national FASD framework could:
- Identify how the federal government, provinces, territories and Indigenous organizations could put in place mechanisms so that these levels of FASD prevention can be offered in a mutually reinforcing way and funded in a coordinated way. Currently at the community level, services struggle to piece together multiple sources of funding so that evidence-based, coordinated, wraparound support can be offered to women and their families, while to date governments have proved incapable of linking their funding programs in order to offer the needed coordination of funding.
- Recommend action for increasing substance use treatment and recovery supports for women who face challenges to reduce or stop problematic substance use, and specifically to increase options for integrated treatment and support for mothers with their children. Women’s treatment options – day treatment, bed-based treatment, and supportive recovery options – are very, very limited in Canada. Such options, where they exist, are not visible and known to be safely accessible by pregnant women and mothers.
- Recommend how research funding into effective practice at each level can be instituted. This could involve specific funding calls from the CIHR and SSHRC, and significant additional funding and leadership for this to be achieved through an enhanced FASD National Strategic Projects Fund and additional efforts from Health Canada and Women and Gender Equality.
- Propose how the federal government could lead work on the awareness raising level through a national campaign as well as link and support regional context- and culturally-specific efforts.
For further information about multi-level prevention, see:
Policy Action
Supportive alcohol policy and child welfare policy are central to the four interconnected levels of prevention. Evidence-based alcohol policies, when widely implemented, have considerable potential to reduce the health and social harms from alcohol, including influencing rates of FASD through each level.
Alcohol policies are critical because they determine the availability of alcohol and other aspects of the environment in which decisions about drinking are made, including how decisions are made in the preconception and perinatal periods. Evidence for the effectiveness of warning labels on alcohol containers and point of sale warning signage in alcohol serving establishments exists, and it is critical that these provide clear and non stigmatizing messages. Other areas of alcohol policy such as outlet restrictions and pricing are also relevant in reducing alcohol and use by all men, women and gender diverse individuals at all times, not only when planning a pregnancy, during pregnancy and when breastfeeding.
Another key alcohol policy strategy is national alcohol-use-in-pregnancy guidelines. These guidelines need to have consistent, updated, evidence-based messaging, and be well known by, and encouraging of action by, all health and social care professionals. Beyond the guidelines themselves, service provider education and practice protocols can promote consistent messaging and foster compassionate understanding of the influences on women’s use, and their preferences for support.
It is particularly important that alcohol policy be linked to child welfare policies and substance use treatment policies that support mother-child togetherness. Such policies can address the barriers that prevent women from seeking care. Instead of gender-blind approaches, policies are needed that promote access to prenatal care, prevent re-traumatization, support priority substance use treatment for pregnant women, support substance use treatment for mothers and children together, and ensure mother-child attachment, all of which have key social returns on investment. Through collaboration and supportive policies across these sectors, women are: able to have healthy pregnancies; supported with early attachment and parenting; linked to treatment and diagnosis as necessary; and able to access services that prioritize women’s goals and address the social and structural determinants of health.
A national FASD framework could:
- Identify and promote action on underdeveloped policy enactment regarding:
- Alcohol policies such as warning labels and point of sale warning signage that promote collective responsibility and support of women to reduce/stop alcohol use in pregnancy in nonstigmatizing ways
- Alcohol guidelines that are sex/gender informed, and support for health and social care providers to learn about and enact such guidance
- Cross system/sector collaboration and policies involving justice, health and child welfare jurisdictions that prevent retraumatization
For further information about alcohol policy action needed:
Prevalence of Alcohol Use in Pregnancy
We live in a society where alcohol is widely available and marketed strongly to women. It is estimated that over 80% of women in Canada drink alcohol, and an estimated 10% of women continue to consume alcohol during pregnancy. Campaigns to raise awareness of the risks of alcohol use for women at all life stages, not only when pregnant have been virtually non-existent in Canada.
We do not have precise data about alcohol use is pregnancy, largely because it is such a highly stigmatized topic:
- Stigma, fear of judgement from health care providers and fear of child apprehension by child welfare authorities prevents women from discussing their alcohol use with health and social care providers.
- Stigma, lack of time, lack of comfort with discussing alcohol, need for training in non-judgemental, compassionate, empowering brief intervention and screening techniques means that providers often do not discuss alcohol with women in the preconception, pregnancy or postpartum period, or do not do so in effective ways.
In order to design effective FASD prevention initiatives, it is important in that we know who is using alcohol in pregnancy – by province/territory, age, income, race, rurality, access to prenatal care, use of other substances, nutritional status, housing status . . . It is critical that those who are not ready or able to stop alcohol use when pregnant have access to health and social care where kind and knowledgeable support is offered. It is important that health and social care providers are able to document alcohol use in ways that support women to get the level and type of assistance they need, without fear of automatic birth alerts and child apprehension.
A national framework could:
- Recommend how health and social care professionals will receive training in evidence-based approaches to discussing alcohol use in pregnancy from national professional bodies, from post secondary education institutions and other avenues to be determined.
- Outline for provincial health authorities how screening and brief intervention can best be achieved and how data on alcohol use by women and in pregnancy can best be collected and shared to inform prevention efforts. It is critical that screening and brief intervention efforts be non-stigmatizing and supportive, based on evidence and policy that values women’s capacity for recovery, trauma informed approaches and mother-child attachment.
- Recommend a mechanism for regular national awareness raising campaigns about the risks of alcohol use by couples, in both the preconception and perinatal periods, and where support is available across the country.
- Ensure a timeline and mechanism for regular updates of national alcohol guidance that outlines the risks of alcohol use for women, men, and gender diverse people overall, as well as in the perinatal period. A mechanism for the funding of knowledge sharing of this evidence-based guidance is needed to support awareness of and actioning of this guidance.
- Recommend regular gathering of maternal experiences such as that done by the Maternity Experiences Survey, funded by PHAC in 2006.
For further detail on establishing prevalence of alcohol use by women:
“Having witnessed firsthand the lifelong challenges faced by individuals with Fetal Alcohol Spectrum Disorder (FASD), I strongly support the initiative to enact a National Framework on FASD. As a biological mother of someone affected by FASD, I understand the profound impact it has on individuals’ brains and bodies, necessitating appropriate lifetime support for their daily living. Through such a framework, we can also work towards ensuring the well-being of both the mother and the unborn child, breaking the cycle of stigma, shame, and judgment that perpetuates the cycle of FASD.”
Janet Christie, Mother and Certified Addiction Recovery Coach
Influences on Alcohol Use in Pregnancy
There are many influences on alcohol use during pregnancy, which means that our approach to prevention must be multifaceted. Key types of influences include:
Structural – Inadequate access to family doctors, to preconception and prenatal care services, as well as contraceptive and substance use services, means that many women do not receive information and support for reducing or stopping alcohol use in childbearing years. Alcohol marketing and lack of uptake of a social responsibility role by Liquor Distribution branches are also societal level influences.
Informational – Access to reliable information about the risks of alcohol use in pregnancy and FASD as a disability is lacking. Misinformation, inconsistent and contradictory messages about safe levels of alcohol and other substance use in pregnancy abound. Women may also not realize they are pregnant and continue to drink in risky ways before pregnancy is recognized.
Stress-related – Common gendered stressors experienced by women such as adverse childhood experiences (ACES), gender-based violence, trauma, mental health concerns, and coercive control by partners are consistently mentioned in the literature as factors contributing to women’s alcohol use, and to dependency on alcohol from using alcohol as means of coping with stress.
Health determinant-related– Social isolation, maternal age, educational attainment, and socioeconomic status (SES) have been identified as influences on alcohol use in pregnancy. While several studies have found that women of older age, higher SES, and higher educational attainment have an increased likelihood of consuming alcohol during pregnancy, other studies have described that younger maternal age, lower SES, and lower educational attainment are linked to increased alcohol consumption during pregnancy.
The range of these influences indicates the critical need for a framework for a comprehensive approach to FASD prevention.
A national framework could:
- Recommend how research funding can be instituted into the structural, informational, stressrelated, health determinant and other influences on women’s alcohol use, and effective strategies for addressing these influences.
- Propose the organization of knowledge sharing forums to be attended by representatives of provinces, territories, Indigenous Nations and organizations and the Public Health Agency of Canada, Health Canada, Corrections Canada and other relevant agencies, where understanding and action on FASD prevention can be discussed and acted on.
For further information on influences on alcohol use in pregnancy, and opportunities to address them see:
Recommendations
Significant social and systemic barriers to accessing appropriate counselling, treatment and basic needs exist when one is pregnant. A national FASD framework would mean Canadians have an evidence-based, nuanced understanding of pregnancy and alcohol-use for more compassionate and supportive communities, and services that are coordinated, responsive, and accessible for pregnant individuals and their future children.
Kristin Bonot, Executive Director, Alberta Parent-Child Assistance Program Council
Bill S-253 identifies the need for a national framework for action on FASD. This brief identifies how a national framework could assist with prevention of FASD, in a way that is supportive of women’s health, in four critically needed areas:
- Advancement in how Canada’s multilevel model of FASD prevention can be further offered, coordinated, funded and researched.
- Promotion of alcohol, child welfare and substance use treatment policies that are equally supportive of women’s health as to children’s health.
- Increase in knowledge of the prevalence and contexts of alcohol use in pregnancy so that prevention programming can best be designed and offered.
- Advancement of research and collaborative action by systems of care that will address the complex influences on women’s substance use in pregnancy.
May you be inspired by the voices and actions of Canadian mothers and service providers described in this brief on this highly stigmatized women’s health and social justice issue, and act on Bill S-253 so that governments and health authorities are catalyzed to expand their understanding and action to support FASD prevention in this country.
Please read the full brief for references.